![]()
![]()
![]()
![]()
|
|
|
|
|
This model implements a 2-tissue compartment model with only two fitted tissue rate constants. It was developed by Choi et al. for cardiac PET studies using 13NH3 ammonia bolus injection and was called the Modified Two-Parameter Model, [47] eq (5).
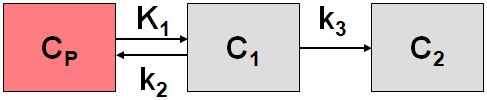
The system of compartmental differential equations for this compartment structure is given by
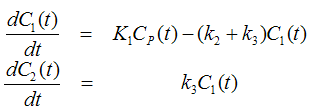
with K1 corresponding to myocardial blood flow (MBF). The k3 rate constant corresponding to glutamine formation was converted into a K1-dependent value by the relation

Similarly, the k2 rate constant of ammonia washout was converted into a K1-dependent value by
![]()
with the V representing the distribution volume of ammonia in the C1 compartment which was assumed to be constant (V=0.8).
In contrast to Choi's method, the model incorporates not only a spillover from the left ventricle, but for septal regions also from the right ventricle. The operational equation is then given by

where
Vlv = spill-over fraction of the blood activity in the left ventricle Clv(t),
Vrv = spill-over fraction of the blood activity in the right ventricle Crv(t) .
Implementation Notes:
Abstract [47]
Several tracer kinetic methods have been proposed for quantification of regional myocardial blood flow (MBF) with 13N-ammonia and PET. Merits and limitations specific to each approach, however, generally are not clear, because they have not been evaluated in the same experimental environment. Therefore, we compared six different commonly used methods (11 modifications) to characterize the accuracy of each approach. The methods included the two-parameter model (method 1), the modified two-parameter model (method 2), the four-parameter model (method 3), the graphical analysis (method 4), the first-pass extraction method (method 5) and the dose uptake index (DUI; method 6). METHODS: Eleven studies in four dogs, 16 studies in eight healthy human volunteers and 14 studies in seven patients were performed using 13N-ammonia and PET. MBF in dogs was varied with dipyridamole and coronary occlusions and was measured independently and simultaneously with microspheres. Volunteers and patients were studied at baseline and after dipyridamole. MBF and DUI were estimated using a time-activity curve (Qi[t]) derived from dynamic images and regions of interest (ROls) and using the six methods. DUI was defined as Qi(t = 2 min) x weight/dose. RESULTS: MBF estimated by methods 1-5 correlated well with microsphere MBF in dogs. MBF estimates by method 1 correlated well with those by methods 2, 4 and 5 and to a lesser degree with those by method 3 in both dog and human studies. DUI correlated poorly with MBF by microspheres and by methods 1-5 in both dog and human studies. MBF estimates by method 3 showed larger dispersion (SD/mean flow) and higher sensitivity to metabolites correction in arterial blood than those by methods 1, 2, 4 and 5. CONCLUSION: MBF can be measured accurately using 13N-ammonia PET and tracer kinetic methods. DUI is a poor indicator of MBF values. The results indicate that preference should be given to the two-parameter model, incorporating geometrical ROI representation (method 2) among the compartment models, and to the graphical analysis (method 4) among the noncompartmental approaches.