![]()
![]()
![]()
![]()
|
|
|
|
|
The model has been implemented according to the method described and evaluated by Herrero et al [35]. Their 82Rb model is based on the following compartment structure to describe the kinetics of rubidium in the myocardium: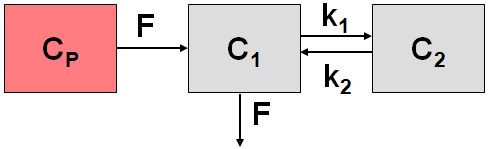
where C1(t) represents the fast exchangeable compartment (vascular and interstitial spaces), and C2(t) the slow exchangeable compartment (intracellular space), myocardium flow F, and rate constants k1 and k2.
The differential equations for the activity concentrations in the different compartments are given by
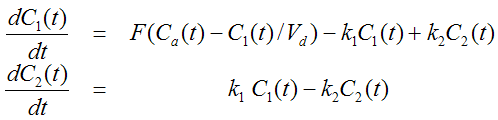
with the arterial blood activity Cp and a fractional volume of distribution Vd in the first compartment .
The operational equation which is fitted to the measured data is
![]()
where FMM denotes the tissue recovery coefficient and the blood to myocardium spillover fraction FBM .
The model encompasses 6 fitable parameters. However, in practice it is impossible to estimate so many parameters from a time-activity curve with reasonable identifiability. Therefore, at least the distribution volume Vd and the recovery coefficient FMM are usually fixed (proposed values from [35]: 0.75 and 0.65 respectively). The recovery coefficient depends on the image resolution and should be determined experimentally.
This model is also usable in the cardiac modeling tool PCARD.
Abstract [35]
"Positron emission tomography offers the ability to noninvasively assess regional myocardial perfusion in absolute terms (i.e., milliliters per gram per minute). Accurate estimates have been difficult to achieve with generator-produced 82Rb because of the complex behavior of this tracer in the myocardium. The aim of the present study was to determine whether regional myocardial blood flow could be assessed quantitatively with 82Rb and positron emission tomography by using a two-compartment kinetic model. Regional perfusion in milliliters per gram per minute was estimated from dynamic tomographic scans after intravenous administration of 82Rb in 18 studies in 13 intact dogs studied without intervention, after 2 and 24 hours of induced ischemia, during reperfusion after transient occlusion, or at rest and after pharmacological hyperemia after induced coronary artery stenosis. Regional flow was estimated along with the forward and backward rates of transport (k1 and k2 [minutes-1]) after the relative volume of distribution of the first compartment was fixed to 0.53 ml/ml and the tomographic parameters, the recovery and spillover fractions, were fixed to averaged values obtained in previous studies. In 36 comparisons, estimates of regional flow with 82Rb correlated well with flow measured with concomitantly administered radiolabeled microspheres (r = 0.91, p less than 0.05) over the flow range from 0.14 to 4.25 ml/g/min. A putative index of viability, k2, increased significantly in regions with severe ischemia. The results suggest that quantification of regional myocardial perfusion is possible in centers using 82Rb for estimates of myocardial perfusion when a physiologically appropriate, two-compartment model is used. Positron emission tomography offers the ability to noninvasively assess regional myocardial perfusion in absolute terms (i.e., milliliters per gram per minute). Accurate estimates have been difficult to achieve with generator-produced 82Rb because of the complex behavior of this tracer in the myocardium. The aim of the present study was to determine whether regional myocardial blood flow could be assessed quantitatively with 82Rb and positron emission tomography by using a two-compartment kinetic model. Regional perfusion in milliliters per gram per minute was estimated from dynamic tomographic scans after intravenous administration of 82Rb in 18 studies in 13 intact dogs studied without intervention, after 2 and 24 hours of induced ischemia, during reperfusion after transient occlusion, or at rest and after pharmacological hyperemia after induced coronary artery stenosis. Regional flow was estimated along with the forward and backward rates of transport (k1 and k2 [minutes-1]) after the relative volume of distribution of the first compartment was fixed to 0.53 ml/ml and the tomographic parameters, the recovery and spillover fractions, were fixed to averaged values obtained in previous studies. In 36 comparisons, estimates of regional flow with 82Rb correlated well with flow measured with concomitantly administered radiolabeled microspheres (r = 0.91, p less than 0.05) over the flow range from 0.14 to 4.25 ml/g/min. A putative index of viability, k2, increased significantly in regions with severe ischemia. The results suggest that quantification of regional myocardial perfusion is possible in centers using 82Rb for estimates of myocardial perfusion when a physiologically appropriate, two-compartment model is used."